Biomedical Computing
Biomedical computing combines the diagnostic and investigative aspects of biology and medical science with the power and problem-solving capabilities of modern computing. Computers are used to accelerate research learning, simulate patient behavior and visualize complex biological models.


Jeff Weiss
Computational Biomechanics
Orly Alter
Computational Biology
Tamara Bidone
Computational Models
Simulations of Biological Systems
Multi-Physics Models of Cancer Cells

Centers and Labs:
- Center for Integrative Biomedical Computing
- Muskuloskeletal Research Laboratory
- Genomic Signal Processing Lab
- Computational Biomechanics Group
Funded Research Projects:
Publications in Biomedical Computing:
  Hip chondrolabral mechanics during activities of daily living: Role of the labrum and interstitial fluid pressurization J.N. Todd, T.G. Maak, G.A. Ateshian, S.A. Maas, J.A. Weiss. In Journal of Biomechanics, Vol. 69, Elsevier BV, pp. 113--120. March, 2018. DOI: 10.1016/j.jbiomech.2018.01.001 Osteoarthritis of the hip can result from mechanical factors, which can be studied using finite element (FE) analysis. FE studies of the hip often assume there is no significant loss of fluid pressurization in the articular cartilage during simulated activities and approximate the material as incompressible and elastic. This study examined the conditions under which interstitial fluid load support remains sustained during physiological motions, as well as the role of the labrum in maintaining fluid load support and the effect of its presence on the solid phase of the surrounding cartilage. We found that dynamic motions of gait and squatting maintained consistent fluid load support between cycles, while static single-leg stance experienced slight fluid depressurization with significant reduction of solid phase stress and strain. Presence of the labrum did not significantly influence fluid load support within the articular cartilage, but prevented deformation at the cartilage edge, leading to lower stress and strain conditions in the cartilage. A morphologically accurate representation of collagen fibril orientation through the thickness of the articular cartilage was not necessary to predict fluid load support. However, comparison with simplified fibril reinforcement underscored the physiological importance. The results of this study demonstrate that an elastic incompressible material approximation is reasonable for modeling a limited number of cyclic motions of gait and squatting without significant loss of accuracy, but is not appropriate for static motions or numerous repeated motions. Additionally, effects seen from removal of the labrum motivate evaluation of labral reattachment strategies in the context of labral repair. |
| P1125 Noninvasive localization of premature ventricular complexes: a research-community-based approach M.J.M. Cluitmans, S. Ghimire, J. Dhamala, J. Coll-Font, J.D. Tate, S. Giffard-Roisin, J. Svehlikova, O. Doessel, M.S. Guillem, D.H. Brooks, R.S. Macleod, L. Wang. In EP Europace, Vol. 20, No. Supplement, Oxford University Press, March, 2018. DOI: 10.1093/europace/euy015.611 Background: Noninvasive localization of premature ventricular complexes (PVCs) to guide ablation therapy is one of the emerging applications of electrocardiographic imaging (ECGI). Because of its increasing clinical use, it is essential to compare the many implementations of ECGI that exist to understand the specific characteristics of each approach. |
| Image-Based Modeling of Acute Myocardial Ischemia Using Experimentally Derived Ischemic Zone Source Representations B.M. Burton, K.K. Aras, W.W. Good, J.D. Tate, B. Zenger, R.S. MacLeod. In Journal of Electrocardiology, Vol. 51, No. 4, Elsevier BV, pp. 725--733. July, 2018. DOI: 10.1016/j.jelectrocard.2018.05.005 Background |
| Higher contact force during radiofrequency ablation leads to a much larger increase in edema as compared to chronic lesion size S. Thomas, J. Silvernagel, N. Angel, E. Kholmovski, E. Ghafoori, N. Hu, J. Ashton, D.J. Dosdall, R.S. MacLeod, R. Ranjan. In Journal of Cardiovascular Electrophysiology, Wiley, June, 2018. DOI: 10.1111/jce.13636 1 Introduction |
| A Framework for Image-Based Modeling of Acute Myocardial Ischemia Using Intramurally Recorded Extracellular Potentials B.M. Burton, K.K. Aras, W.W. Good, J.D. Tate, B. Zenger, R.S. MacLeod. In Annals of Biomedical Engineering, Springer Nature, May, 2018. DOI: 10.1007/s10439-018-2048-0 The biophysical basis for electrocardiographic evaluation of myocardial ischemia stems from the notion that ischemic tissues develop, with relative uniformity, along the endocardial aspects of the heart. These injured regions of subendocardial tissue give rise to intramural currents that lead to ST segment deflections within electrocardiogram (ECG) recordings. The concept of subendocardial ischemic regions is often used in clinical practice, providing a simple and intuitive description of ischemic injury; however, such a model grossly oversimplifies the presentation of ischemic disease—inadvertently leading to errors in ECG-based diagnoses. Furthermore, recent experimental studies have brought into question the subendocardial ischemia paradigm suggesting instead a more distributed pattern of tissue injury. These findings come from experiments and so have both the impact and the limitations of measurements from living organisms. Computer models have often been employed to overcome the constraints of experimental approaches and have a robust history in cardiac simulation. To this end, we have developed a computational simulation framework aimed at elucidating the effects of ischemia on measurable cardiac potentials. To validate our framework, we simulated, visualized, and analyzed 226 experimentally derived acute myocardial ischemic events. Simulation outcomes agreed both qualitatively (feature comparison) and quantitatively (correlation, average error, and significance) with experimentally obtained epicardial measurements, particularly under conditions of elevated ischemic stress. Our simulation framework introduces a novel approach to incorporating subject-specific, geometric models and experimental results that are highly resolved in space and time into computational models. We propose this framework as a means to advance the understanding of the underlying mechanisms of ischemic disease while simultaneously putting in place the computational infrastructure necessary to study and improve ischemia models aimed at reducing diagnostic errors in the clinic. |
| Computationally optimized ECoG stimulation with local safety constraints S. Guler, M. Dannhauer, B. Roig-Solvas, A. Gkogkidis, R. Macleod, T. Ball, J. G. Ojemann, D. H. Brooks. In NeuroImage, Vol. 173, Elsevier BV, pp. 35--48. June, 2018. DOI: 10.1016/j.neuroimage.2018.01.088 Direct stimulation of the cortical surface is used clinically for cortical mapping and modulation of local activity. Future applications of cortical modulation and brain-computer interfaces may also use cortical stimulation methods. One common method to deliver current is through electrocorticography (ECoG) stimulation in which a dense array of electrodes are placed subdurally or epidurally to stimulate the cortex. However, proximity to cortical tissue limits the amount of current that can be delivered safely. It may be desirable to deliver higher current to a specific local region of interest (ROI) while limiting current to other local areas more stringently than is guaranteed by global safety limits. Two commonly used global safety constraints bound the total injected current and individual electrode currents. However, these two sets of constraints may not be sufficient to prevent high current density locally (hot-spots). In this work, we propose an efficient approach that prevents current density hot-spots in the entire brain while optimizing ECoG stimulus patterns for targeted stimulation. Specifically, we maximize the current along a particular desired directional field in the ROI while respecting three safety constraints: one on the total injected current, one on individual electrode currents, and the third on the local current density magnitude in the brain. This third set of constraints creates a computational barrier due to the huge number of constraints needed to bound the current density at every point in the entire brain. We overcome this barrier by adopting an efficient two-step approach. In the first step, the proposed method identifies the safe brain region, which cannot contain any hot-spots solely based on the global bounds on total injected current and individual electrode currents. In the second step, the proposed algorithm iteratively adjusts the stimulus pattern to arrive at a solution that exhibits no hot-spots in the remaining brain. We report on simulations on a realistic finite element (FE) head model with five anatomical ROIs and two desired directional fields. We also report on the effect of ROI depth and desired directional field on the focality of the stimulation. Finally, we provide an analysis of optimization runtime as a function of different safety and modeling parameters. Our results suggest that optimized stimulus patterns tend to differ from those used in clinical practice. |
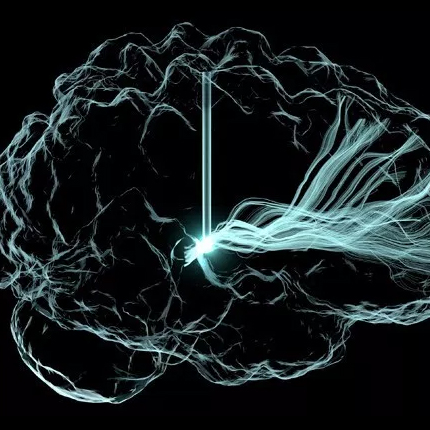
| Optimized programming algorithm for cylindrical and directional deep brain stimulation electrodes D. N. Anderson, B. Osting, J. Vorwerk, A. D Dorval, C. R Butson. In Journal of Neural Engineering, Vol. 15, No. 2, pp. 026005. 2018. Objective. Deep brain stimulation (DBS) is a growing treatment option for movement and psychiatric disorders. As DBS technology moves toward directional leads with increased numbers of smaller electrode contacts, trial-and-error methods of manual DBS programming are becoming too time-consuming for clinical feasibility. We propose an algorithm to automate DBS programming in near real-time for a wide range of DBS lead designs. Approach. Magnetic resonance imaging and diffusion tensor imaging are used to build finite element models that include anisotropic conductivity. The algorithm maximizes activation of target tissue and utilizes the Hessian matrix of the electric potential to approximate activation of neurons in all directions. We demonstrate our algorithm's ability in an example programming case that targets the subthalamic nucleus (STN) for the treatment of Parkinson's disease for three lead designs: the Medtronic 3389 (four cylindrical contacts), the direct STNAcute (two cylindrical contacts, six directional contacts), and the Medtronic-Sapiens lead (40 directional contacts). Main results. The optimization algorithm returns patient-specific contact configurations in near real-time—less than 10 s for even the most complex leads. When the lead was placed centrally in the target STN, the directional leads were able to activate over 50% of the region, whereas the Medtronic 3389 could activate only 40%. When the lead was placed 2 mm lateral to the target, the directional leads performed as well as they did in the central position, but the Medtronic 3389 activated only 2.9% of the STN. Significance. This DBS programming algorithm can be applied to cylindrical electrodes as well as novel directional leads that are too complex with modern technology to be manually programmed. This algorithm may reduce clinical programming time and encourage the use of directional leads, since they activate a larger volume of the target area than cylindrical electrodes in central and off-target lead placements. |
| Research and Education in Computational Science and Engineering U. Ruede, K. Willcox, L. C. McInnes, H. De Sterck, G. Biros, H. Bungartz, J. Corones, E. Cramer, J. Crowley, O. Ghattas, M. Gunzburger, M. Hanke, R. Harrison, M. Heroux, J. Hesthaven, P. Jimack, C. Johnson, K. E. Jordan, D. E. Keyes, R. Krause, V. Kumar, S. Mayer, J. Meza, K. M. Mrken, J. T. Oden, L. Petzold, P. Raghavan, S. M. Shontz, A. Trefethen, P. Turner, V. Voevodin, B. Wohlmuth,, C. S. Woodward. In SIAM Review, Vol. 60, No. 3, SIAM, pp. 707--754. Jan, 2018. DOI: 10.1137/16m1096840 This report presents challenges, opportunities and directions for computational science and engineering (CSE) research and education for the next decade. Over the past two decades the field of CSE has penetrated both basic and applied research in academia, industry, and laboratories to advance discovery, optimize systems, support decision-makers, and educate the scientific and engineering workforce. Informed by centuries of theory and experiment, CSE performs computational experiments to answer questions that neither theory nor experiment alone is equipped to answer. CSE provides scientists and engineers with algorithmic inventions and software systems that transcend disciplines and scales. CSE brings the power of parallelism to bear on troves of data. Mathematics-based advanced computing has become a prevalent means of discovery and innovation in essentially all areas of science, engineering, technology, and society; and the CSE community is at the core of this transformation. However, a combination of disruptive developments—including the architectural complexity of extreme-scale computing, the data revolution and increased attention to data-driven discovery, and the specialization required to follow the applications to new frontiers—is redefining the scope and reach of the CSE endeavor. With these many current and expanding opportunities for the CSE field, there is a growing demand for CSE graduates and a need to expand CSE educational offerings. This need includes CSE programs at both the undergraduate and graduate levels, as well as continuing education and professional development programs, exploiting the synergy between computational science and data science. Yet, as institutions consider new and evolving educational programs, it is essential to consider the broader research challenges and opportunities that provide the context for CSE education and workforce development. |
| Characterization of Gadolinium Contrast Enhancement of Radiofrequency Ablation Lesions in Predicting Edema and Chronic Lesion Size E. Ghafoori, E.G. Kholmovski, S. Thomas, J. Silvernagel, N. Angel, N. Hu, D.J. Dosdall, R.s. MacLeod, R. Ranjan. In Circulation: Arrhythmia and Electrophysiology, Vol. 10, No. 11, Ovid Technologies (Wolters Kluwer Health), pp. e005599. Oct, 2017. DOI: 10.1161/circep.117.005599 Background Magnetic resonance imaging (MRI) has been used to acutely visualize radiofrequency ablation lesions, but its accuracy in predicting chronic lesion size is unknown. The main goal of this study was to characterize different areas of enhancement in late gadolinium enhancement MRI done immediately after ablation to predict acute edema and chronic lesion size. |
| Detecting Ischemic Stress to the Myocardium Using Laplacian Eigenmaps and Changes to Conduction Velocity W. W. Good, B. Erem, J. Coll-Font, D. H. Brooks, R. S. MacLeod. In Computing in Cardiology, Vol. 44, IEEE, 2017. The underlying pathophysiology of ischemia and its electrocardiographic consequences are poorly understood, resulting in unreliable diagnosis of this disease. This limited knowledge of underlying mechanisms suggests a data driven approach, which seeks to identify patterns in the ECG that can be linked statistically to underlying behavior and conditions of ischemic stress. The gold standard ECG metrics for evaluating ischemia monitor vertical deflections within the ST segment. However, ischemia influences all portions of the electrogram. Another metric that targets the QRS complex during ischemia is Conduction Velocity (CV). An even more inclusive, data driven approach is known as "Laplacian Eigenmaps" (LE), which can identify trajectories, or "manifolds", that respond to different spatiotemporal consequences of ischemic stress, and these changes to the trajectories on the manifold may serve as a clinically relevant biomarker. On this study, we compared the LE- and CV-based markers against two gold standards for detecting ischemic stress, both derived from the ST segment. We evaluated the response time and fidelity of each biomarker using a Time to Threshold (TTT) and Contrast Ratio (CR) measure, over 51 episodes recorded as cardiac electrograms from a canine model of controlled ischemia. The results show that metrics designed to monitor regions beyond the ST segment can perform at least as well, if not better, than traditional ST segment based metrics. |
| Analyzing Source Sampling to Reduce Error in ECG Forward Simulations J. Tate, K. Gillette, B. Burton, W. Good, J. Coll-Font, D. Brooks, R. MacLeod. In Computing in Cardiology, Vol. 44, 2017. A continuing challenge in validating ECG Imaging is the persistent error in the associated forward problem observed in experimental studies. One possible cause of error is insufficient representation of the cardiac sources, which is often measured from only the ventricular epicardium, ignoring the endocardium and the atria. We hypothesize that measurements that completely cover the heart are required for accurate forward solutions. In this study, we used simulated and measured cardiac potentials to test the effect of different levels of sampling on the forward simulation. We found that omitting source samples on the atria increases the peak RMS error by a mean of 464 μV when compared the the fully sampled cardiac surface. Increasing the sampling on the atria in stages reduced the average error of the forward simulation proportionally to the number of additional samples and revealed some strategies may reduce error with fewer samples, such as adding samples to the AV plane and the atrial roof. Based on these results, we can design a sampling strategy to use in future validation studies. |
| Overcoming Barriers to Quantification and Comparison of Electrocardiographic Imaging Methods: A Community-Based Approach S. Ghimire, J. Dhamala, J. Coll-Font, J. D. Tate, M. S. Guillem, D. H. Brooks, R. S. MacLeod, L. Wang. In Computing in Cardiology, Vol. 44, 2017. There has been a recent upsurge in the development of electrocardiographic imaging (ECGI) methods, along with a significant increase in clinical application. To better assess the state-of-the-art, enable reliable progress, and facilitate clinical adoption, it is important to be able to compare results in a comprehensive manner, scientifically and clinically. However, studies vary in modeling choices, computational methods, validation mechanisms and metrics, and clinical applications, making unified evaluation and comparison of ECGI a critical challenge. |
| ECG-Based Reconstruction of Heart Position and Orientation with Bayesian Optimization J. Coll-Font, S. Ariafar, D. H Brooks. In Computing in Cardiology, Vol. 44, 2017. Respiratory motion is known to cause beat-to-beat variation of the ECG. This observation suggests that it may be possible to use this variation to track position and orientation of the heart. Electrocardiographic Imaging (ECGI) would benefit from such a reconstruction since one contribution to errors in its solutions is respiratory motion of the heart. ECGI solutions generally rely on prior computation of a "forward" model that relates cardiac electrical activity to ECGs. However, the ill-posed nature of the inverse solution leads to large errors in ECGI even for small amounts of error in the forward model. The current work is a first step towards reducing those errors using a nominal forward model and the ECG itself. We describe a method that can reconstruct cardiac position / orientation using known potentials on both the heart and torso. Our current implementation is based on Bayesian Optimization and efficiently optimizes for the position / orientation of the heart to minimize error between measured and forward-computed torso potentials. We evaluated our approach with synthesized torso potentials under a model of respiratory motion and also using potentials recorded in a tank experiment on a canine epicardium and the tank surfaces. Our results show that our method performs accurately in synthetic experiments and can account for part of the error between forward-computed and measured ECGs in the tank experiments. |
| Pedunculopontine nucleus deep brain stimulation in Parkinson's disease: A clinical review W.Thevathasan, B. Debu, T. Aziz, B. R. Bloem, C. Blahak, C. Butson, V. Czernecki, T. Foltynie, V. Fraix, D. Grabli, C. Joint, A. M. Lozano, M. S. Okun, J. Ostrem, N. Pavese, C. Schrader, C. H. Tai, J. K. Krauss, E. Moro. In Movement Disorders, Vol. 33, No. 1, pp. 10--20. 2017. ISSN: 1531-8257 DOI: 10.1002/mds.27098 Pedunculopontine nucleus region deep brain stimulation (DBS) is a promising but experimental therapy for axial motor deficits in Parkinson's disease (PD), particularly gait freezing and falls. Here, we summarise the clinical application and outcomes reported during the past 10 years. The published dataset is limited, comprising fewer than 100 cases. Furthermore, there is great variability in clinical methodology between and within surgical centers. The most common indication has been severe medication refractory gait freezing (often associated with postural instability). Some patients received lone pedunculopontine nucleus DBS (unilateral or bilateral) and some received costimulation of the subthalamic nucleus or internal pallidum. Both rostral and caudal pedunculopontine nucleus subregions have been targeted. However, the spread of stimulation and variance in targeting means that neighboring brain stem regions may be implicated in any response. Low stimulation frequencies are typically employed (20-80 Hertz). The fluctuating nature of gait freezing can confound programming and outcome assessments. Although firm conclusions cannot be drawn on therapeutic efficacy, the literature suggests that medication refractory gait freezing and falls can improve. The impact on postural instability is unclear. Most groups report a lack of benefit on gait or limb akinesia or dopaminergic medication requirements. The key question is whether pedunculopontine nucleus DBS can improve quality of life in PD. So far, the evidence supporting such an effect is minimal. Development of pedunculopontine nucleus DBS to become a reliable, established therapy would likely require a collaborative effort between experienced centres to clarify biomarkers predictive of response and the optimal clinical methodology. |
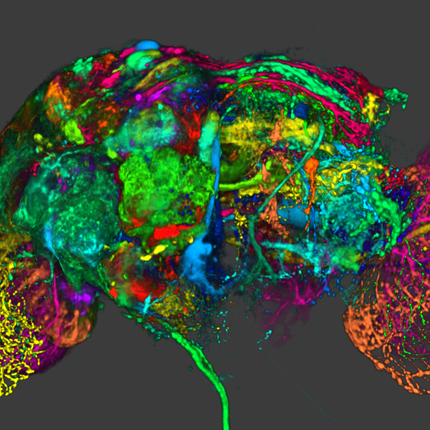
| FluoRender: joint freehand segmentation and visualization for many-channel fluorescence data analysis Y. Wan, H. Otsuna, H. A. Holman, B. Bagley, M. Ito, A. K. Lewis, M. Colasanto, G. Kardon, K. Ito, C. Hansen. In BMC Bioinformatics, Vol. 18, No. 1, Springer Nature, May, 2017. DOI: 10.1186/s12859-017-1694-9 Background: |
| Uncertainty Footprint: Visualization of Nonuniform Behavior of Iterative Algorithms Applied to 4D Cell Tracking Y. Wan, C. Hansen. In Computer Graphics Forum, Wiley, 2017. Research on microscopy data from developing biological samples usually requires tracking individual cells over time. When cells are three-dimensionally and densely packed in a time-dependent scan of volumes, tracking results can become unreliable and uncertain. Not only are cell segmentation results often inaccurate to start with, but it also lacks a simple method to evaluate the tracking outcome. Previous cell tracking methods have been validated against benchmark data from real scans or artificial data, whose ground truth results are established by manual work or simulation. However, the wide variety of real-world data makes an exhaustive validation impossible. Established cell tracking tools often fail on new data, whose issues are also difficult to diagnose with only manual examinations. Therefore, data-independent tracking evaluation methods are desired for an explosion of microscopy data with increasing scale and resolution. In this paper, we propose the uncertainty footprint, an uncertainty quantification and visualization technique that examines nonuniformity at local convergence for an iterative evaluation process on a spatial domain supported by partially overlapping bases. We demonstrate that the patterns revealed by the uncertainty footprint indicate data processing quality in two algorithms from a typical cell tracking workflow – cell identification and association. A detailed analysis of the patterns further allows us to diagnose issues and design methods for improvements. A 4D cell tracking workflow equipped with the uncertainty footprint is capable of self diagnosis and correction for a higher accuracy than previous methods whose evaluation is limited by manual examinations. |
| Proceedings of the Fourth Annual Deep Brain Stimulation Think Tank: A Review of Emerging Issues and Technologies W. Deeb, J. J. Giordano, P. J. Rossi, A. Y. Mogilner, A. Gunduz, J. W. Judy, B. T. Klassen, C. R. Butson, C. Van Horne, D. Deny, D. D. Dougherty, D. Rowell, G. A. Gerhardt, G. S. Smith, F. A. Ponce, H. C. Walker, H. M. Bronte-Stewart, H. S. Mayberg, H. J. Chizeck, J. Langevin, J. Volkmann, J. L. Ostrem, J. B. Shute, J. Jimenez-Shahed, K. D. Foote, A. W. Shukla, M. A. Rossi, M. Oh, M. Pourfar, P. B. Rosenberg, P. A. Silburn, C. de Hemptine, P. A. Starr, T. Denison, U. Akbar, W. M. Grill,, M. S. Okun. In Frontiers in Integrative Neuroscience, Vol. 10, pp. 38. 2016. ISSN: 1662-5145 DOI: 10.3389/fnint.2016.00038 This paper provides an overview of current progress in the technological advances and the use of deep brain stimulation (DBS) to treat neurological and neuropsychiatric disorders, as presented by participants of the Fourth Annual Deep Brain Stimulation Think Tank, which was convened in March 2016 in conjunction with the Center for Movement Disorders and Neurorestoration at the University of Florida, Gainesveille FL, USA. The Think Tank discussions first focused on policy and advocacy in DBS research and clinical practice, formation of registries, and issues involving the use of DBS in the treatment of Tourette Syndrome. Next, advances in the use of neuroimaging and electrochemical markers to enhance DBS specificity were addressed. Updates on ongoing use and developments of DBS for the treatment of Parkinson’s disease, essential tremor, Alzheimer’s disease, depression, post-traumatic stress disorder, obesity, addiction were presented, and progress toward innovation(s) in closed-loop applications were discussed. Each section of these proceedings provides updates and highlights of new information as presented at this year’s international Think Tank, with a view toward current and near future advancement of the field. |
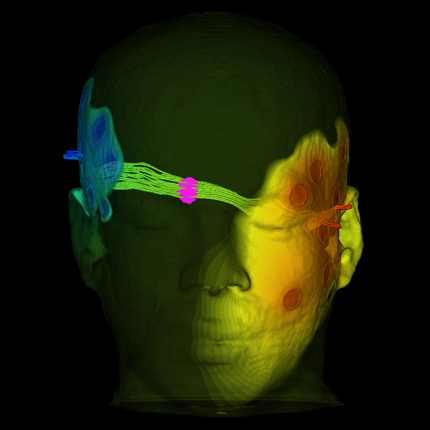
| Alternating Current Stimulation for Vision Restoration after Optic Nerve Damage: A Randomized Clinical Trial C. Gall, S. Schmidt, M.P. Schittkowski, A. Antal, G. Ambrus, W. Paulus, M. Dannhauer, R. Michalik, A. Mante, M. Bola, A. Lux, S. Kropf, S.A. Brandt, B.A. Sabel. In PLOS ONE, Vol. 11, No. 6, Public Library of Science, pp. e0156134. June, 2016. DOI: 10.1371/journal.pone.0156134 Background |
| Robust modulation of arousal regulation, performance, and frontostriatal activity through central thalamic deep brain stimulation in healthy nonhuman primates J.L. Baker, J. Ryou, X.F. Wei, C.R. Butson, N.D. Schiff, K.P. Purpura. In Journal of Neurophysiology, Vol. 116, No. 5, American Physiological Society, pp. 2383--2404. Aug, 2016. DOI: 10.1152/jn.01129.2015 The central thalamus (CT) is a key component of the brain-wide network underlying arousal regulation and sensory-motor integration during wakefulness in the mammalian brain. Dysfunction of the CT, typically a result of severe brain injury (SBI), leads to long-lasting impairments in arousal regulation and subsequent deficits in cognition. Central thalamic deep brain stimulation (CT-DBS) is proposed as a therapy to reestablish and maintain arousal regulation to improve cognition in select SBI patients. However, a mechanistic understanding of CT-DBS and an optimal method of implementing this promising therapy are unknown. Here we demonstrate in two healthy nonhuman primates (NHPs), Macaca mulatta, that location-specific CT-DBS improves performance in visuomotor tasks and is associated with physiological effects consistent with enhancement of endogenous arousal. Specifically, CT-DBS within the lateral wing of the central lateral nucleus and the surrounding medial dorsal thalamic tegmental tract (DTTm) produces a rapid and robust modulation of performance and arousal, as measured by neuronal activity in the frontal cortex and striatum. Notably, the most robust and reliable behavioral and physiological responses resulted when we implemented a novel method of CT-DBS that orients and shapes the electric field within the DTTm using spatially separated DBS leads. Collectively, our results demonstrate that selective activation within the DTTm of the CT robustly regulates endogenous arousal and enhances cognitive performance in the intact NHP; these findings provide insights into the mechanism of CT-DBS and further support the development of CT-DBS as a therapy for reestablishing arousal regulation to support cognition in SBI patients. |
| Longitudinal Changes in Depressive Circuitry in Response to Neuromodulation Therapy Y. Pathak, O. Salami, S. Baillet, Z. Li, C.R. Butson. In Frontiers in Neural Circuits, Vol. 10, rontiers Media SA, July, 2016. DOI: 10.3389/fncir.2016.00050 BACKGROUND: |